
It feels like a family reunion, but we’ve never met these people before. But just like at a family reunion, there are lots of people that look a lot like each other and have the same ears and mouth.
People that have the same sense of humor and make the same gestures. And just like in families, there are people with the same health conditions, both physical and mental.
Those are like blood relatives that we are spending time with these days.
In the more extended family, there is less resemblance, but they are connected through contact with the blood like relatives.
The extended family cracks jokes that only they are allowed to make and outsiders cannot. The extended family loves the blood like relatives and shares hopes and sorrows and can sometimes understand each other without words.
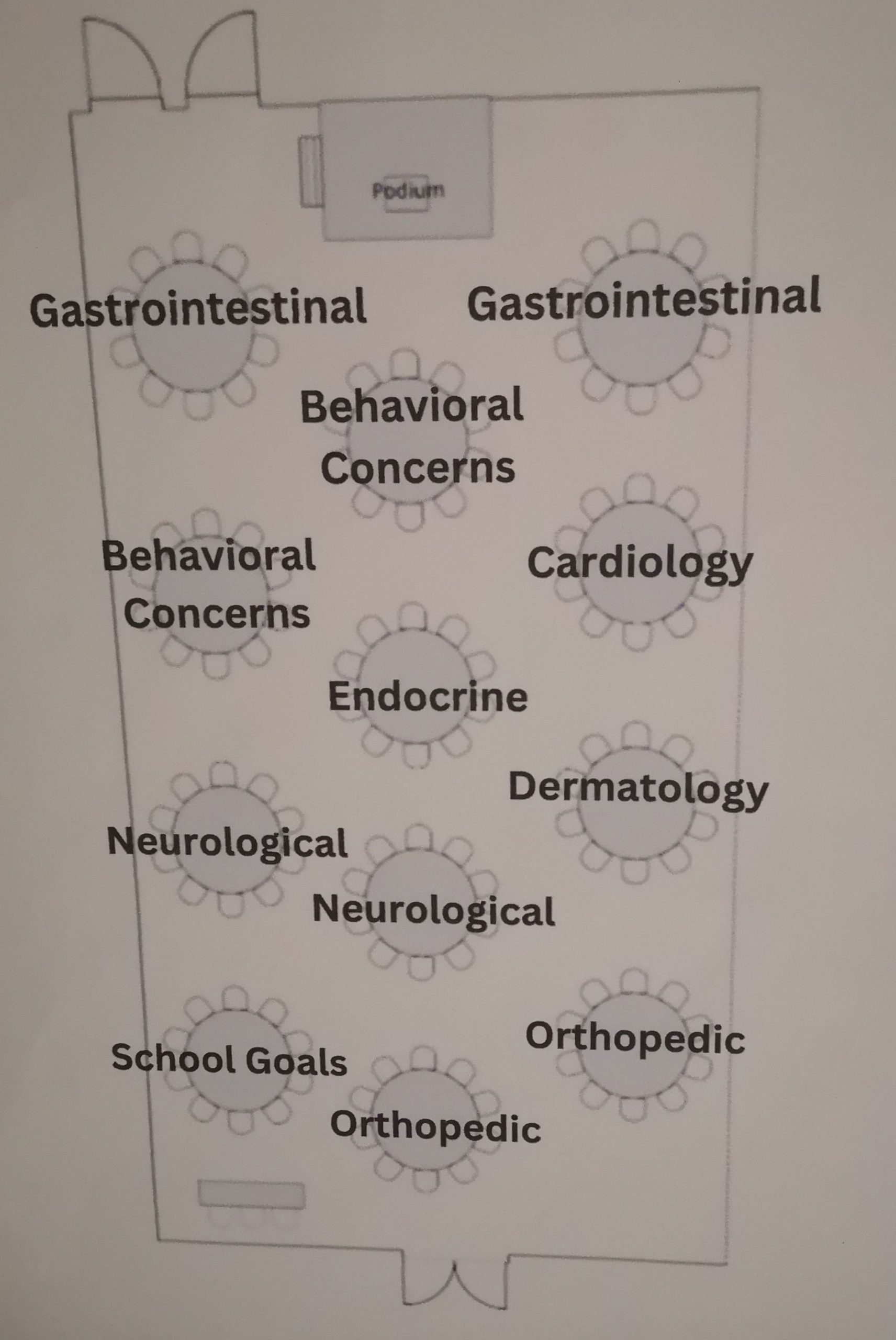
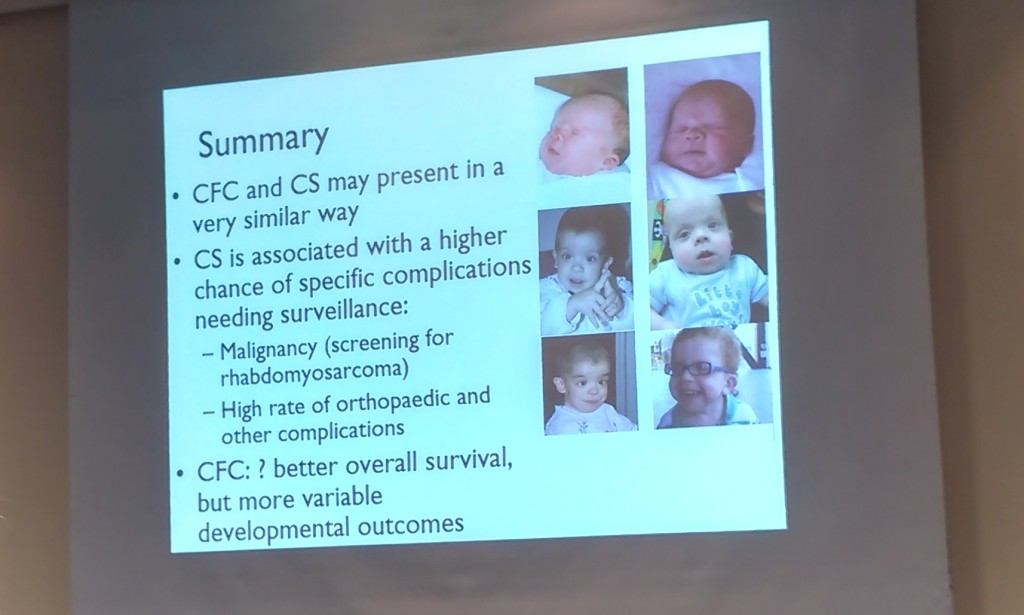
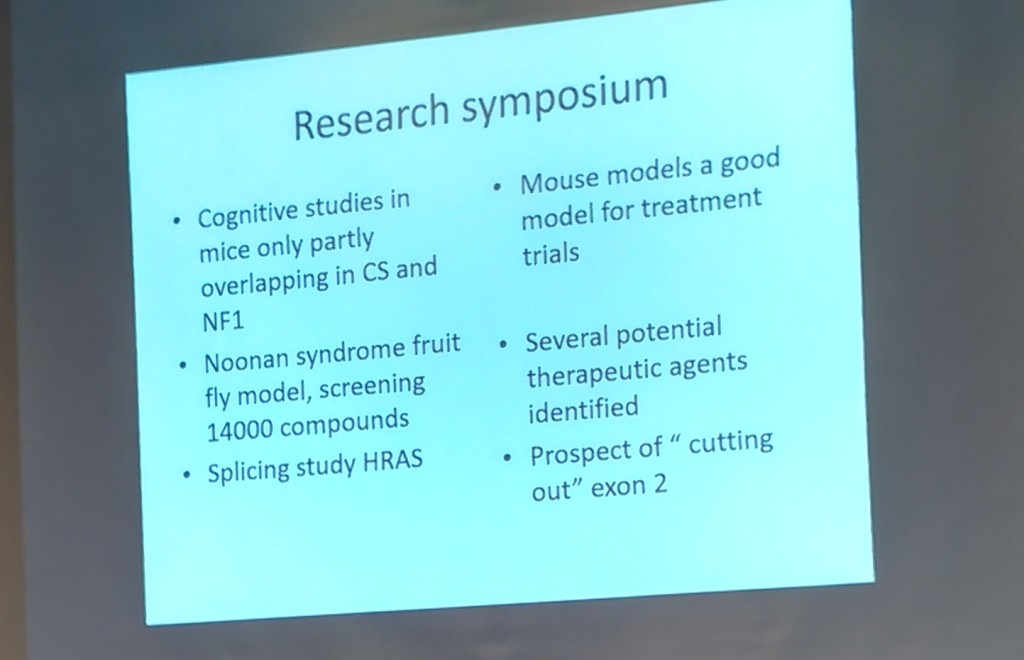
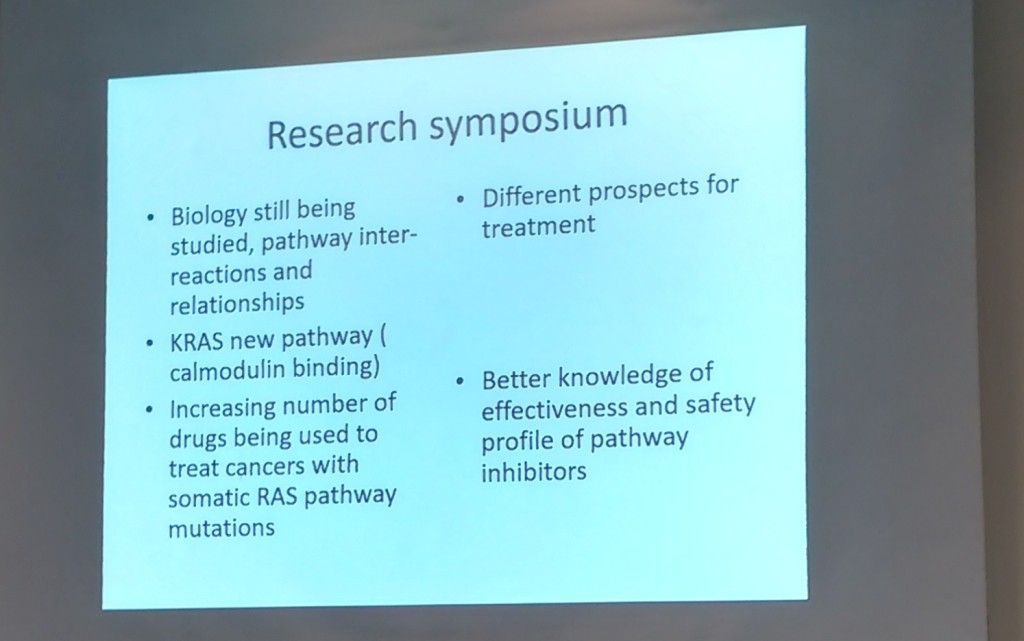
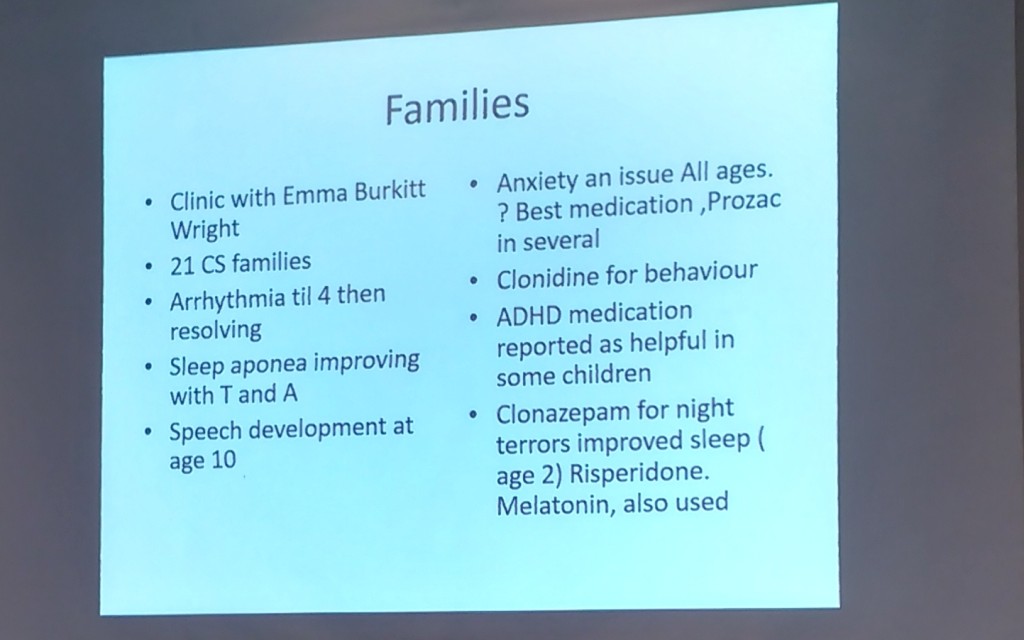
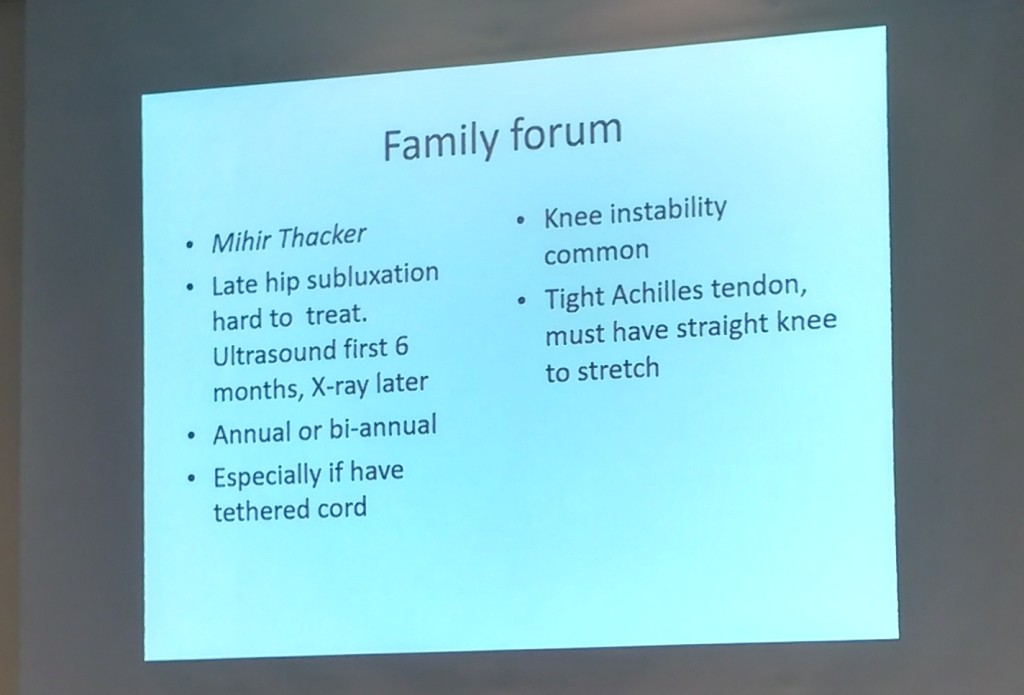
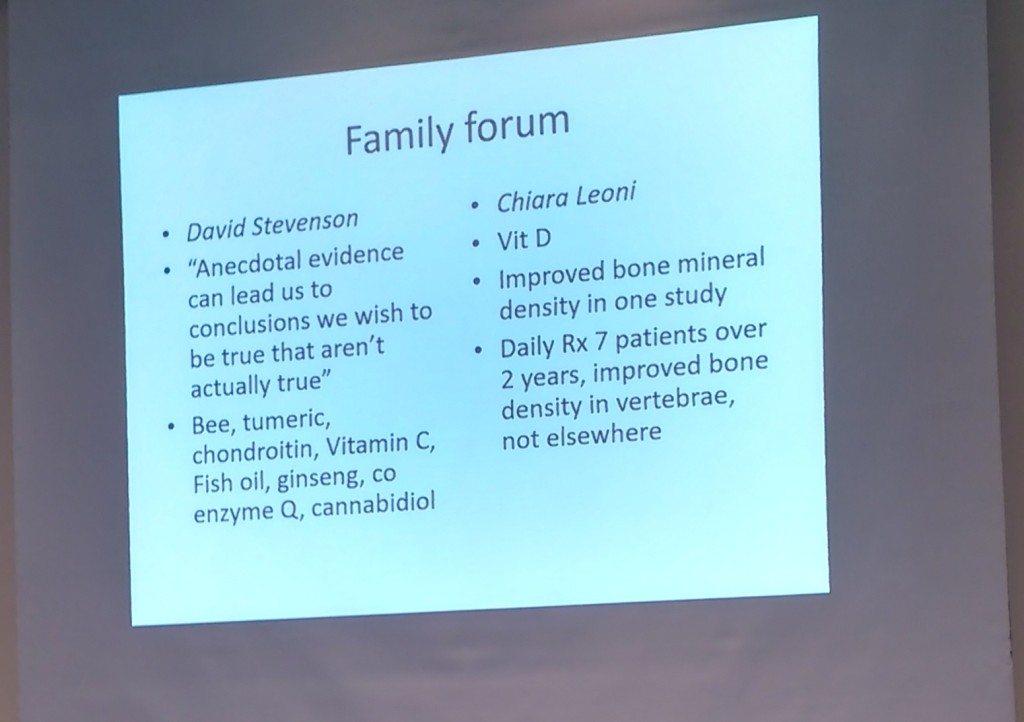
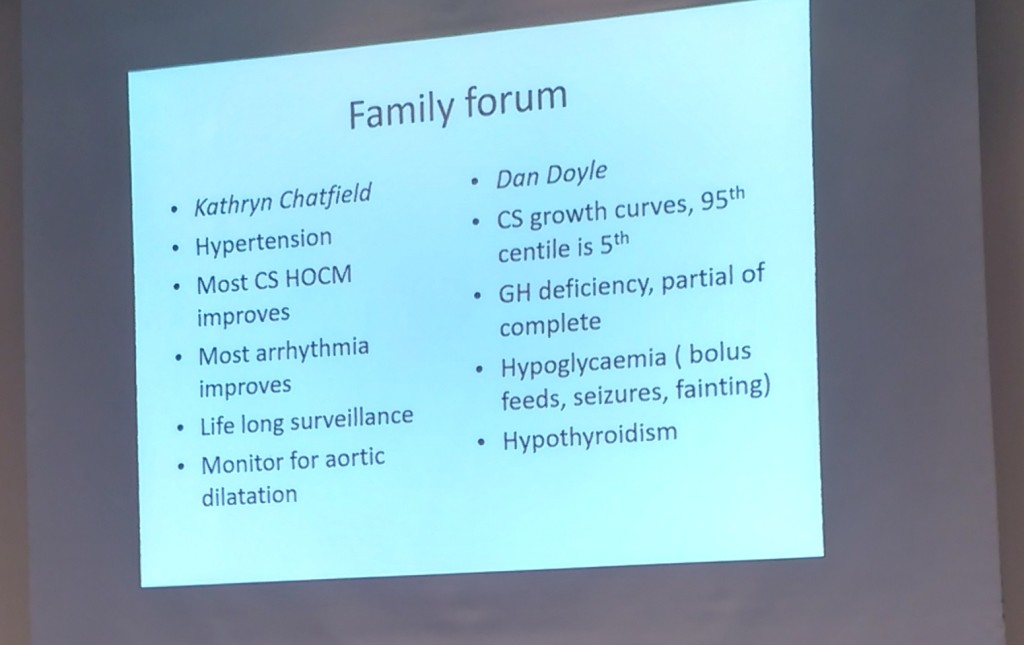
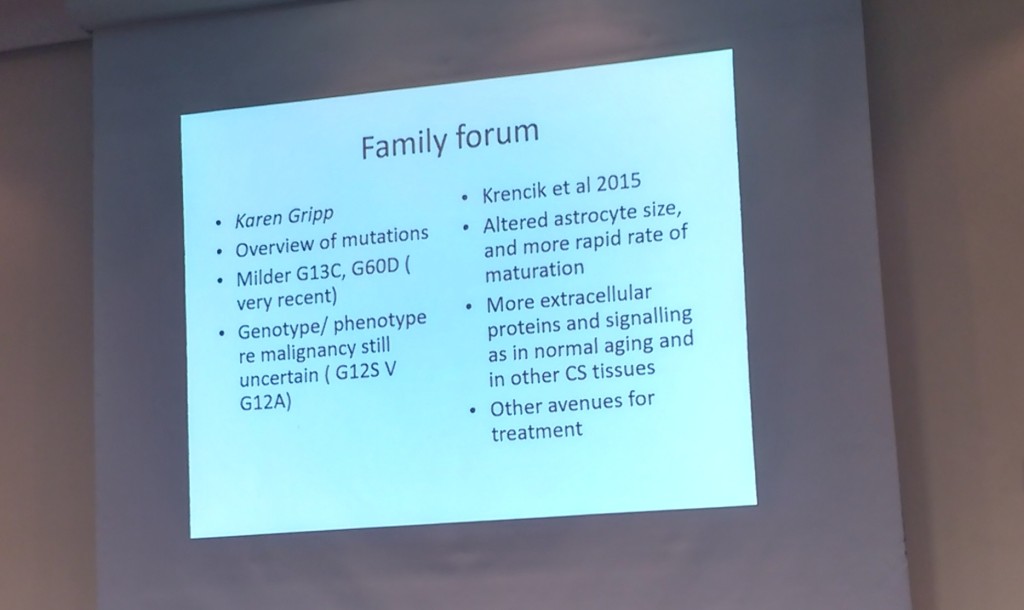
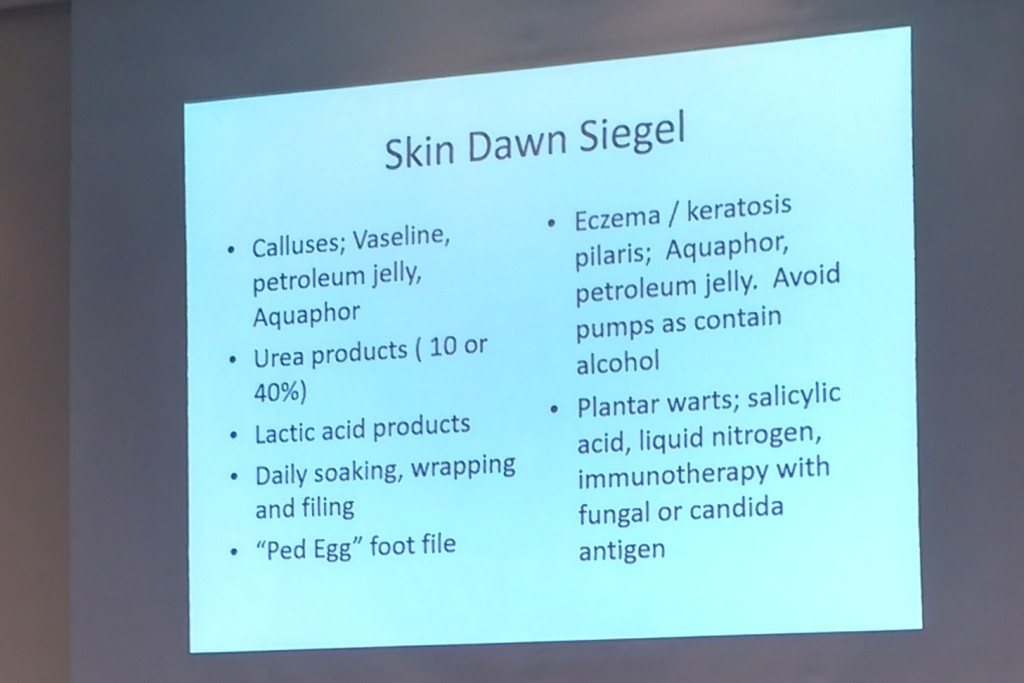
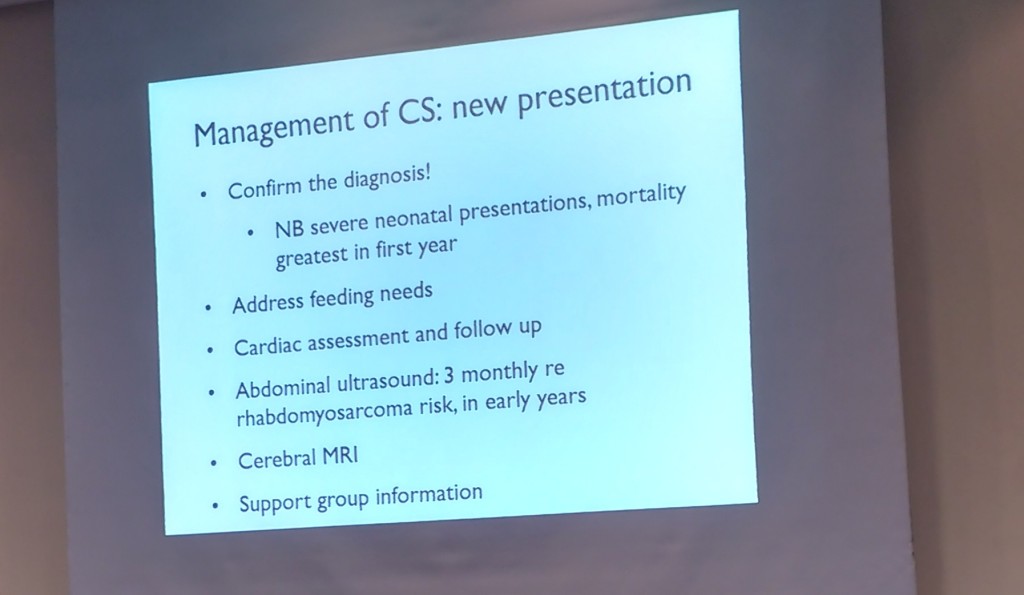
Together, this one big family is made up of people with Costello syndrome. This summer, our family spent time with 45 other families at the international convention in Denver, USA. We had been looking forward to this for years and now the time had come. We experienced 4 special days with a substantive program. There was an introductory day, an afternoon for siblings, a men’s evening, a day full of lectures by medical specialists, a women’s evening, a day for meeting with specialists to ask questions regarding our individual situations, a memorial space full of candles and photos of those who are no longer with us, a day for roundtable discussions and a festive party night.
We ate meals together, we talked, we laughed, gave each other hugs for encouragement, took pictures. We soaked up all the information to use as tools to help us interact with our own person with Costello. Sometimes this information makes us sad and worried because so many health issues could crop up. It makes us think, makes us alert and often confirms what we already know and experience. All this acknowledgment and recognition feels good to all of us.

We are happily surprised that Mieke lands in a wonderful international group of siblings that connected from day 1. They roam through the halls of the hotel, snapchat, hang out and dance together.
We notice Vera is more aware of her identity and that Costello syndrome is a part of that. Sometimes she becomes overwhelmed with how many people there are. She meets other girls that look so much like her, they could be cousins. And even though there is a language barrier, it feels nice to be around each other.

We take a dive in the hotel pool and revel in the fact that no one is staring at us, like at most public swimming pools. But we do notice the scars that we all have. Scars that tell stories of illness and surgeries that Vera has endured as well or may be in her future, some we hope to avoid. We play in the water to release some sensory overstimulation and enjoy ourselves.
And before we know it, these days are over. We leave the hotel and continue to enjoy another two weeks of vacation and family visit. We have lots more adventures and push our limits. And we are thankful for the beautiful people, gorgeous nature, nice weather and for the fact that we are all healthy during this trip. Such a blessing and wonderful relaxation.

Now we are home again in Gouda, The Netherlands. We get back in the swing of things with school and work. We look at the pictures and have started sharing everything we’ve learned with local Dutch Costello families, as well as Vera’s specialists and therapists. On the inside, a warm feeling of connection remains. And no amount of kilometers or flight hours can change that.